Childhood Acute Myeloid Leukemia/Other Myeloid Malignancies Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Acute Myeloid Leukemia and Other Myeloid Malignancies
Childhood acute myeloid leukemia (AML) is a type of cancer in which the bone marrow makes a large number of abnormal blood cells.
Childhood acute myeloid leukemia (AML) is a cancer of the blood and bone marrow. AML is also called acute myelogenous leukemia and acute nonlymphocytic leukemia. Cancers that are acute usually get worse quickly if they are not treated. Cancers that are chronic usually get worse slowly.
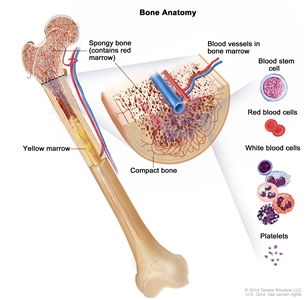
Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
This summary is about the treatment of childhood AML, transient abnormal myelopoiesis, childhood acute promyelocytic leukemia, juvenile myelomonocytic leukemia, childhood chronic myelogenous leukemia, and childhood myelodysplastic syndromes. For information about the treatment of childhood acute lymphoblastic leukemia, see Childhood Acute Lymphoblastic Leukemia Treatment.
Leukemia and other diseases of the blood and bone marrow may affect red blood cells, white blood cells, and platelets.
In healthy children, the bone marrow makes blood stem cells (immature cells) that become mature blood cells over time. A blood stem cell may become a myeloid stem cell or a lymphoid stem cell. A lymphoid stem cell becomes a type of white blood cell.
A myeloid stem cell becomes one of three types of mature blood cells:
- Red blood cells that carry oxygen and other substances to all tissues of the body.
- Granulocytes, which are white blood cells that help fight infection and disease.
- Platelets that form blood clots to stop bleeding.
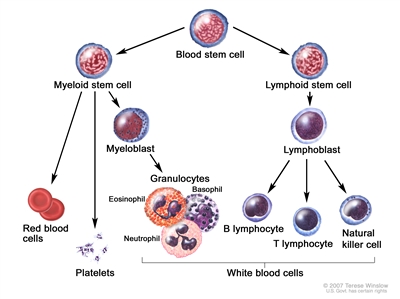
Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
In AML, the myeloid stem cells usually become a type of immature white blood cell called myeloblasts (or myeloid blasts). The myeloblasts, or leukemia cells, in AML are abnormal and do not become healthy white blood cells. The leukemia cells can build up in the blood and bone marrow so there is less room for healthy white blood cells, red blood cells, and platelets. This may lead to infection, anemia, or easy bleeding.
The leukemia cells can spread outside the blood to other parts of the body, including the central nervous system (brain and spinal cord), skin, and gums. Sometimes leukemia cells form a solid tumor called a myeloid sarcoma. Myeloid sarcoma is also called granulocytic sarcoma or chloroma.
Other myeloid diseases can affect the blood and bone marrow.
Transient abnormal myelopoiesis (TAM)
TAM is a disorder of the bone marrow that can develop in newborns who have Down syndrome. TAM usually goes away on its own within the first 3 months of life. Infants who have TAM have an increased chance of developing AML before the age of 3 years. TAM is also called transient myeloproliferative disorder or transient leukemia.
Acute promyelocytic leukemia (APL)
APL is a subtype of AML. In APL, some genes on chromosome 15 switch places with some genes on chromosome 17 and an abnormal gene called PML-RARA is made. The PML-RARA gene sends a message that stops promyelocytes (a type of white blood cell) from maturing. The promyelocytes (leukemia cells) can build up in the blood and bone marrow so there is less room for healthy white blood cells, red blood cells, and platelets. Problems with severe bleeding and blood clots may also occur. This is a serious health problem that needs treatment as soon as possible.
Juvenile myelomonocytic leukemia (JMML)
JMML is a rare childhood cancer that is most common in children around the age of 2 years and is more common in boys. In JMML, too many myeloid blood stem cells become myelocytes and monocytes (two types of white blood cells). Some of these myeloid blood stem cells never become mature white blood cells. These immature cells, called blasts, are unable to do their usual work. Over time, the myelocytes, monocytes, and blasts crowd out the healthy white blood cells, red blood cells, and platelets in the bone marrow. When this happens, infection, anemia, or easy bleeding may occur.
Chronic myelogenous leukemia (CML)
CML often begins in an early myeloid blood cell when a certain gene change occurs. A section of genes, that includes the ABL gene, on chromosome 9 changes place with a section of genes on chromosome 22, which has the BCR gene. This makes a very short chromosome 22 (called the Philadelphia chromosome) and a very long chromosome 9. An abnormal BCR-ABL gene is formed on chromosome 22. The BCR-ABL gene tells the blood cells to make too much of a protein called tyrosine kinase. Tyrosine kinase causes too many abnormal white blood cells (leukemia cells) to be made in the bone marrow. The leukemia cells can build up in the blood and bone marrow so there is less room for healthy white blood cells, red blood cells, and platelets. This can lead to infection, anemia, or easy bleeding. CML is rare in children.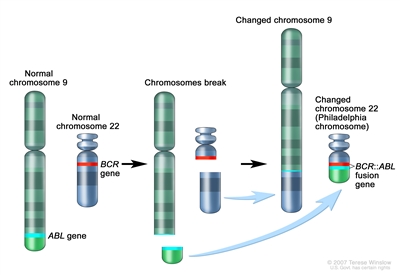
The Philadelphia (Ph) chromosome is an abnormal chromosome that is made when pieces of chromosomes 9 and 22 break off and trade places. The ABL gene from chromosome 9 joins to the BCR gene on chromosome 22 to form the BCR::ABL fusion gene. The changed chromosome 22 with the fusion gene on it is called the Ph chromosome.
Myelodysplastic syndromes (MDS)
MDS occur less often in children than in adults. In MDS, the bone marrow makes too few red blood cells, white blood cells, and platelets. These blood cells may not mature and enter the blood. The type of MDS depends on the type of blood cell that is affected.
The treatment for MDS depends on how low the numbers of red blood cells, white blood cells, or platelets are. Over time, MDS may become AML.
AML or MDS may occur after treatment with certain chemotherapy drugs and/or radiation therapy.
Cancer treatment with certain chemotherapy drugs and/or radiation therapy may cause therapy-related AML (t-AML) or therapy -related MDS (t-MDS). The risk of these therapy-related myeloid diseases depends on the total dose of the chemotherapy drugs used and the radiation dose and treatment field. Some patients also have an inherited risk for t-AML and t-MDS. These therapy-related diseases usually occur within 7 years after treatment, but are rare in children.
The risk factors for childhood acute myeloid leukemia and other myeloid malignancies are similar.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your child's doctor if you think your child may be at risk. These and other factors may increase the risk of childhood AML, APL, JMML, CML, and MDS:
- Having a brother or sister, especially a twin, with leukemia.
- Having a personal history of bone marrow failure.
- Having a personal history of MDS.
- Past treatment with chemotherapy or radiation therapy.
- Being exposed to ionizing radiation or chemicals such as benzene.
- Having certain syndromes or inherited disorders, such as:
- Down syndrome.
- Aplastic anemia.
- Fanconi anemia.
- Neurofibromatosis type 1.
- Noonan syndrome.
- Shwachman-Diamond syndrome.
- Diamond-Blackfan anemia.
- Dyskeratosis congenita.
- Li-Fraumeni syndrome.
Signs and symptoms of childhood acute myeloid leukemia and other myeloid malignancies include fever, feeling tired, and easy bleeding or bruising.
These and other signs and symptoms may be caused by childhood AML, APL, JMML, CML, or MDS or by other conditions. Check with a doctor if your child has any of the following:
- Fever with or without an infection.
- Drenching night sweats.
- Shortness of breath.
- Weakness, feeling tired, or looking pale.
- Easy bruising or bleeding.
- Petechiae (flat, pinpoint spots under the skin caused by bleeding).
- Bone or joint pain.
- Pain or feeling of fullness below the ribs.
- Painless lumps in the neck, underarm, stomach, groin, or other parts of the body. In childhood AML, these lumps, called leukemia cutis, may be blue or purple.
- Painless lumps that are sometimes around the eyes. These lumps, called myeloid sarcomas, are sometimes seen in childhood AML and may be blue-green.
- An eczema -like skin rash.
- Loss of appetite or weight loss.
- Headache, trouble seeing, or confusion.
The signs and symptoms of TAM may include the following:
- Swelling all over the body.
- Shortness of breath.
- Trouble breathing.
- Increased heart rate.
- Weakness, feeling tired, or looking pale.
- Easy bleeding or bruising.
- Petechiae (flat, pinpoint spots under the skin caused by bleeding).
- Pain below the ribs.
- Skin rash.
- Jaundice (yellowing of the skin and whites of the eyes).
Sometimes TAM does not cause any symptoms at all and is diagnosed after a routine blood test.
Tests that examine the blood and bone marrow are used to diagnose and find any spread of childhood acute myeloid leukemia and other myeloid malignancies.
The following tests and procedures may be used:
- Physical exam and health history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
-
Complete blood count (CBC) with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells and platelets.
- The number and type of white blood cells.
- The portion of the blood sample made up of red blood cells.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
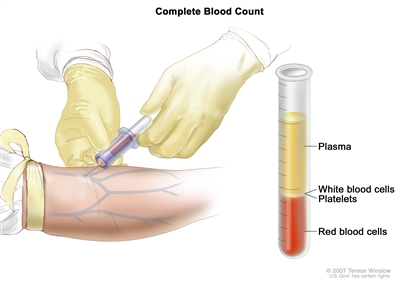
Complete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions. - Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
-
Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. Biopsies that may be done include the following:
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone.
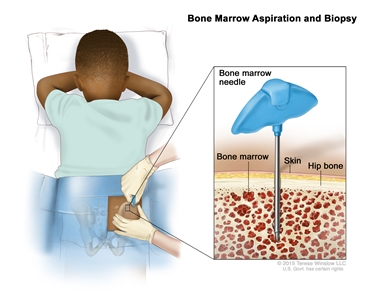
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child's hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope. - Tumor biopsy for AML: The removal of cells or tissues from a lump in the testicles, ovaries, or skin using a needle. This may be done if the doctor suspects the leukemia cells may have formed a solid tumor called a myeloid sarcoma.
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone.
- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of leukemia.
-
Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of blood or bone marrow are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
The following test is a type of cytogenetic analysis:
- FISH (fluorescence in situ hybridization): A laboratory test used to look at and count genes or chromosomes in cells and tissues. Pieces of DNA that contain fluorescent dyes are made in the laboratory and added to a sample of a patient's cells or tissues. When these dyed pieces of DNA attach to certain genes or areas of chromosomes in the sample, they light up when viewed under a fluorescent microscope. The FISH test is used to help diagnose cancer and help plan treatment.
- Molecular testing: A laboratory test to check for certain genes, proteins, or other molecules in a sample of tissue, blood, or bone marrow. Molecular tests also check for certain changes in a gene or chromosome that may cause or affect the chance of developing AML. A molecular test may be used to help plan treatment, find out how well treatment is working, or make a prognosis.
-
Lumbar puncture: A procedure used to collect a sample of cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs that leukemia cells have spread to the brain and spinal cord. This procedure is also called an LP or spinal tap.
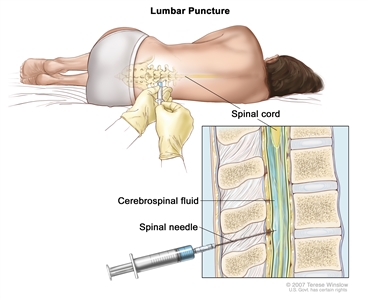
Lumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options for childhood acute myeloid leukemia (AML) depend on the following:
- The age of the child when the cancer is diagnosed.
- The race or ethnic group of the child.
- Whether the child is greatly overweight.
- Number of white blood cells in the blood at diagnosis.
- Whether the AML occurred after previous cancer treatment.
- The subtype of AML.
- Whether there are certain chromosome or gene changes in the leukemia cells.
- Whether the child has Down syndrome. Most children with AML and Down syndrome can be cured of their leukemia when diagnosed before age 4 years.
- Whether the leukemia is in the central nervous system (brain and spinal cord).
- How quickly the leukemia responds to treatment.
- Whether the AML is newly diagnosed (untreated) or has recurred after treatment.
- The length of time since treatment ended, for AML that has recurred.
The prognosis and treatment options for childhood acute promyelocytic leukemia (APL) depends on the following:
- Number of white blood cells in the blood at diagnosis.
- Whether there are certain chromosome or gene changes in the leukemia cells.
- Whether the APL is newly diagnosed (untreated) or has recurred after treatment.
The prognosis and treatment options for juvenile myelomonocytic leukemia (JMML) depend on the following:
- The age of the child when the cancer is diagnosed.
- The type of gene affected and the number of genes that have changes.
- How many platelets are in the blood after treatment.
- How much hemoglobin is in the blood after treatment.
- Whether the JMML is newly diagnosed (untreated) or has recurred after treatment.
The prognosis and treatment options for childhood chronic myelogenous leukemia (CML) depend on the following:
- How long it has been since the patient was diagnosed.
- How many blast cells are in the blood.
- Whether and how fully the blast cells disappear from the blood and bone marrow after therapy has started.
- Whether the CML is newly diagnosed (untreated) or has recurred after treatment.
The prognosis and treatment options for myelodysplastic syndromes (MDS) depend on the following:
- Whether the MDS was caused by previous cancer treatment.
- How low the numbers of red blood cells, white blood cells, or platelets are.
- Whether the MDS is newly diagnosed (untreated) or has recurred after treatment.
Treatment Option Overview
There are different types of treatment for children with acute myeloid leukemia and other myeloid malignancies.
Different types of treatment are available for children with acute myeloid leukemia (AML), transient abnormal myelopoiesis (TAM), acute promyelocytic leukemia (APL), juvenile myelomonocytic leukemia (JMML), chronic myelogenous leukemia (CML), and myelodysplastic syndromes (MDS). Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Because AML and other myeloid disorders are rare in children, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not yet started treatment.
Treatment is planned by a team of health care providers who are experts in treating childhood leukemia and other diseases of the blood.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other health care providers who are experts in treating children with leukemia and who specialize in certain areas of medicine. These may include the following specialists:
- Pediatrician.
- Hematologist.
- Medical oncologist.
- Pediatric surgeon.
- Radiation oncologist.
- Neurologist.
- Neuropathologist.
- Neuroradiologist.
- Pediatric nurse specialist.
- Social worker.
- Rehabilitation specialist.
- Psychologist.
The treatment of childhood AML and other myeloid malignancies usually has two phases.
The treatment of childhood AML is done in phases:
- Induction therapy: This is the first phase of treatment. The goal is to kill the leukemia cells in the blood and bone marrow. This puts the leukemia into remission.
- Consolidation /intensification therapy: This is the second phase of treatment. It begins once the leukemia is in remission. The goal of therapy is to kill any remaining leukemia cells that are hiding and may not be active but could begin to regrow and cause a relapse.
Treatment called central nervous system (CNS) prophylaxis therapy may be given during the induction phase of therapy. Because standard doses of chemotherapy may not reach leukemia cells in the CNS (brain and spinal cord), the leukemia cells are able to hide in the CNS. Intrathecal chemotherapy is able to reach leukemia cells in the CNS. It is given to kill the leukemia cells and lessen the chance the leukemia will recur (come back).
The treatment of childhood APL includes a third phase called maintenance. The goal of maintenance is to kill any remaining leukemia cells that may regrow and cause a relapse. Often the cancer treatments are given in lower doses than those used during the remission induction and consolidation/intensification phases.
Seven types of standard treatment may be used for childhood AML and other myeloid malignancies.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid (intrathecal chemotherapy), an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is treatment using more than one chemotherapy drug.
The way the chemotherapy is given depends on the type of cancer being treated. In AML, chemotherapy given by mouth, vein, or into the cerebrospinal fluid is used.
In AML, the leukemia cells may spread to the brain and/or spinal cord. Chemotherapy given by mouth or vein to treat AML may not cross the blood-brain barrier to get into the fluid that surrounds the brain and spinal cord. Instead, chemotherapy is injected into the fluid-filled space to kill leukemia cells that may have spread there (intrathecal chemotherapy).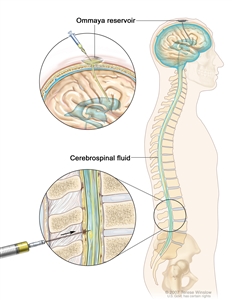
Intrathecal chemotherapy. Anticancer drugs are injected into the intrathecal space, which is the space that holds the cerebrospinal fluid (CSF, shown in blue). There are two different ways to do this. One way, shown in the top part of the figure, is to inject the drugs into an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). The other way, shown in the bottom part of the figure, is to inject the drugs directly into the CSF in the lower part of the spinal column, after a small area on the lower back is numbed.
See Drugs Approved for Acute Myeloid Leukemia for more information.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer.
In childhood AML, external radiation therapy may be used to treat a myeloid sarcoma that does not respond to chemotherapy.
Stem cell transplant
Chemotherapy is given to kill cancer cells or other abnormal blood cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
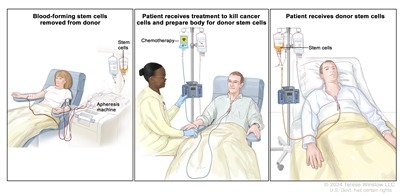
Donor stem cell transplant. (Step 1): Four to five days before donor stem cell collection, the donor receives a medicine to increase the number of stem cells circulating through their bloodstream (not shown). The blood-forming stem cells are then collected from the donor through a large vein in their arm. The blood flows through an apheresis machine that removes the stem cells. The rest of the blood is returned to the donor through a vein in their other arm. (Step 2): The patient receives chemotherapy to kill cancer cells and prepare their body for the donor stem cells. The patient may also receive radiation therapy (not shown). (Step 3): The patient receives an infusion of the donor stem cells.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do. Types of targeted therapy include the following:
-
Tyrosine kinase inhibitor therapy: This treatment blocks the enzyme, tyrosine kinase, that causes stem cells to become more white blood cells (blasts) than the body needs. Tyrosine kinase inhibitors may be used with chemotherapy drugs as adjuvant therapy (treatment given after the initial treatment, to lower the risk that the cancer will come back).
- Imatinib, dasatinib, and nilotinib are used to treat childhood chronic myelogenous leukemia.
- Sorafenib, midostaurin, and gilteritinib, which target a mutated (changed) form of a gene called FLT3, are being studied to treat childhood AML.
- Trametinib is being studied in children with recurrent or refractory juvenile myelomonocytic leukemia.
-
Monoclonal antibodies: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
- Gemtuzumab ozogamicin is a type of monoclonal antibody that is attached to a chemotherapy drug. It is used in the treatment of AML.
See Drugs Approved for Leukemia for more information.
Other drug therapy
Lenalidomide may be used to lessen the need for transfusions in patients who have myelodysplastic syndromes caused by a specific chromosome change.
Arsenic trioxide and tretinoin are drugs that kill certain types of leukemia cells, stop the leukemia cells from dividing, or help the leukemia cells mature into white blood cells. These drugs are used in the treatment of acute promyelocytic leukemia.
See Drugs Approved for Acute Myeloid Leukemia for more information.
Watchful waiting
Watchful waiting is closely monitoring a patient's condition without giving any treatment until signs or symptoms appear or change. It is sometimes used to treat transient abnormal myelopoiesis (TAM).
Supportive care
Supportive care is given to lessen the problems caused by the disease or its treatment. All patients with leukemia receive supportive care treatments. Supportive care may include the following:
- Transfusion therapy: A way of giving red blood cells or platelets to replace blood cells destroyed by disease or cancer treatment. The blood may be donated from another person or it may have been taken from the patient earlier and stored until needed.
- Antifungal agents: Drugs, such as Caspofungin or fluconazole, used to prevent or treat infections caused by a fungus (a type of microorganism). This is important in the care of patients with AML.
- Drug therapy, such as antibiotics.
- Leukapheresis: A procedure in which a special machine is used to remove white blood cells from the blood. Blood is taken from the patient and put through a blood cell separator where the white blood cells are removed. The rest of the blood is then returned to the patient's bloodstream. Leukapheresis is used to treat patients with very high white blood cell counts.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Treatment for childhood acute myeloid leukemia and other myeloid malignancies may cause side effects.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Regular follow-up exams are very important. Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include the following:
- Physical problems that affect the following:
- Heart, lung, or endocrine function.
- Bone development.
- Fertility (ability to have children).
- Energy level.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer), such as breast cancer.
Some late effects may be treated or controlled. It is important that parents of children who are treated for AML or other blood diseases talk with their child's doctors about the effects cancer treatment can have on their child. (See the PDQ summary on Late Effects of Treatment for Childhood Cancer for more information).
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back).

